Any rapid growth of cells in an aberrant pattern in the brain that results in the creation of atypical tissue is called neoplasm. One of the prominent types of neoplasm is an Astrocytoma.
Certain types of star-shaped cells, which are called glial cells, are the source of origination of an Astrocytoma.
This type of tumor is also referred to as glioma because of its inception from the glial cells. The spread of a tumor of this nature is usually found in the brain and sometimes on the spinal cord.

A Brain Tumor

Microscopic View of an Astrocytoma
Astrocytomas are classified into two main categories:
- Ones with constricted zones of penetration, namely, pilocytic, pleomorphic xanthoastrocytoma and subependymal giant cell astrocytoma. These can be clearly identified in diagnostic representations.
- The other type of Astrocytoma is scattered in nature and could be dispersed in any area of the brain or spinal cord. For instance, low-grade astrocytoma, anaplastic astrocytoma, and glioblastoma. These tumors have the tendency to appear and grow anywhere in the central nervous system, largely in the cerebral hemispheres. Their occurrence is usually found in adults, and they have an inherent propensity to progressively worsen into complex formations. This kind of Astrocytoma is called Malignant Astrocytoma.
The term malignant is used medically for any severe and increasingly aggravating disease, usually cancer. The characteristic property of this kind of neoplasm is to grow continuously and infiltrate into surrounding healthy tissues.
Malignant Astrocytoma is observed to occur at any age. The low-grade tumor is common in children and adolescents, while high-grade tumor is known to develop in adults.
Glioblastoma multiforme (GBM) is the most ordinary and the most malignant form of astrocytoma.

A grade IV Malignant Astrocytoma – GBM
A Malignant Astrocytoma manifests as:
1) Anaplastic astrocytomas – This is a grade III type of astrocytoma according to the grading system devised by WHO. Surgical removal and subsequent radiation treatment are the most commonly employed forms of treatment for this type of Malignant Astrocytoma. A patient has an average survival time of up to 18 months after the implementation of prescribed treatment.
2) Glioblastoma multiforme (GBM) – This is the most common form of Malignant Astrocytoma. It is characterized by rapid growth of cells and their spread to healthy brain tissues. Usually even before a patient shows any symptoms, its size and diffusion in the brain might become so pronounced that chances of complete surgical removal diminish completely. It can manifest as abrupt seizures or as an intense headache.
Not even 10% of GBM are a result of deterioration of grade I, II or III astrocytoma. These are referred to as secondary GBM and are commonly found in patients with an average age of 45. Elimination of the tumor by operation is the most preferred option for this type of GBM only if injury to the neurological system can be averted.
Even though radiation therapy is rarely known to heal glioblastoma totally, research has proven that it doubles the average survival of patients as compared to administering only supportive care.
The prospects are worst for a grade IV Malignant Astrocytoma or GBM. Very few patients survive for more than 3 years.
Patients with a grade IV Malignant Astrocytoma have an average survival period of a little over 4 months without any treatment, around 7 months with radiation therapy, and about 9 months post-removal of the tumor via surgical procedure, followed by a personalized treatment plan comprised of radiation therapy and chemotherapy.
Less than 3% of these patients survive for approximately 5 years.
Symptoms
There are several symptoms associated with a Malignant Astrocytoma
-
- Occurrence of frequent, unexplained headaches
- Rise in intracranial stress
- Frequent nausea and early-morning vomiting
- Inexplicable changes in behaviour and personality
- Recurrent forgetfulness
- Thwarted intellectual reactions
- Occurrence of seizures, fits or spasms
- A paralysis attack
- Deterioration in the ability to write — agraphia
- A pins-and-needles prickling or piercing sensation
- Loss of perception of one’s being or existence in space — proprioception
- Lack of coordination in muscular movements
- Sudden poor language interpretation

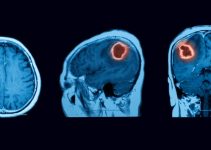
A CT Scan of a Malignant Astrocytoma
Causes of Occurrence
The exact reason why a Malignant Astrocytoma develops is unknown, however, both hereditary and environmental factors have been postulated. In particular, a person’s DNA may have undergone mutation due to a previous history of radiation exposure due to treatment for any past disease, resulting in unrestrained cell multiplication.
This disease is more commonly found in males as compared to females. Since contagiousness has no relation with genetics or heredity, this disease is not known to spread through any infection.
Treatment – Malignant Astrocytoma
Astrocytomas manifest as various types and in varying grades. Their location in the brain and the extent of spread might differ from case to case. A patient’s health history and biological age are also decisive in determining the correct mode of treatment for a Malignant Astrocytoma.
If the astrocytoma is in its initial stage and is low-grade, its surgical elimination will result in a patient's survival for several years. Reports say that 90% of cases have shown normal body function for at least five years after a successful surgery in a low-grade astrocytoma.
Predominantly, Pilocytic astrocytomas are known to be mostly inactive and allow normal functioning of the CNS in most cases. However, if disregarded these may assume neoplasmic form, so surgical removal and subsequent regular monitoring is the course of action.
So far, total removal of a high-grade Malignant Astrocytoma is unattainable because by the time the tumor is detected, it has generally spread to various normal parts of the brain in the form of patches of tissues. Even after surgery or therapy, there are very high chances that the tumor may show recurrence.
Providing symptomatic relief is the best doctors can do at the advanced stage of a Malignant Astrocytoma.
A professional, well-planned treatment would consist of the following:
- Medication to relieve the prevalent symptoms.
- Surgical removal, depending on the position and spread of the tumor.
- Chemotherapy – oral Temozolomide or intravenous injections, usually administered in degenerated form of disease and in some cases in the initial stages as well.
There is no established exactitude of the causes of occurrence of a Malignant Astrocytoma and hence no recognized preventive measures.
According to the data published by WHO, grade I astrocytoma contributes a mere 2% to all reported astrocytomas, 8% is contributed by grade II, and the grade III Anaplastic Astrocytomas amount to 20%. Grade IV Astrocytoma — Malignant GBM — is the most commonly occurring cancer of the nervous system and the next most common brain tumor following metastasis of the brain.
Despite the lesser prevalence of astrocytomas in comparison to various other cancers, grades III & IV have demonstrated high mortality, owing to untimely detection of the tumor due to its lack of manifestation via symptoms.
Finally, since the ideal treatment plan is impossible to devise and considering the brief nature of patients’ responses, experimental trials of latest advancements in medicinal research should be employed and encouraged.